
nederlands
“Periodontal EDS” is also known as pEDS, EDS type VIII, Ehlers-Danlos Syndrome periodontitis type or Ehlers-Danlos Syndrome periodontosis type (11).
This specific subtype was first described by McKusick in 1972 as a “unique condition“ in a patient with EDS-like features, such as lesions on the shins, slow-healing brakes in the skin, atrophic scars and absorptive periodontitis including early loss of teeth. Only five years later, in 1977, Stewart et al. publicized a similar case and defined this variant as EDS VIII. Subsequently another 32 cases of pEDS and 7 pedigree analyses have been reported (11,12).
It is important to state that “periodontal EDS“ is a specific disease. It is not to be mistaken with a patient suffering from another EDS subtype like classical or hypermobile EDS who additionally is affected by periodontitis. With up to 80% in the adult population, periodontitis has a very high prevalence; therefore, a coincidence with any EDS subtype is possible.
Clinical oral features of the autosomal-dominant disease periodontal EDS include extensive inflammation of the gingiva as a result of mild dental plaque accumulation as well as early and severe periodontitis that goes hand in hand with rapid destruction of the attachment apparatus at juvenile age (13).
This early and severe periodontits is the hallmark of pEDS and with gingival recession the defining clinical feature. If the patients don’t receive periodontal treatment these individuals have a great chance of being edentulous at a mean age of 20 years.

Typical recessions with missing attached gingiva and thin mucosa © Ines Kapferer-Seebacher

Typical recessions with missing attached gingiva and thin mucosa © Ines Kapferer-Seebacher

Child with missing attached gingiva and thin mucosa, gingival inflammation in the lower jaw with mild plaque © Ines Kapferer-Seebacher

© Ines Kapferer-Seebacher
The defining extraoral feature of pEDS is pretibial hyperpigmentation while other characteristica include easy bruising, skin fragility, and mild skin hyperextensibility. Joint hypermobility is restricted to small joints (13). These pretibial hyperpigmentations are a consequence of easy bruising, delayed wound healing as well as tissue fragility to an injury prone body area.
This fragility is often complicated by a variable bleeding tendency. These manifestations have often been misdiagnosed as child abuse, which underlines the importance of gathering detailed family and personal history (14).
Leg ulcer is a typical manifestation and may occur within these brownish pretibial plaques because of tissue fragility and delayed wound healing (15).
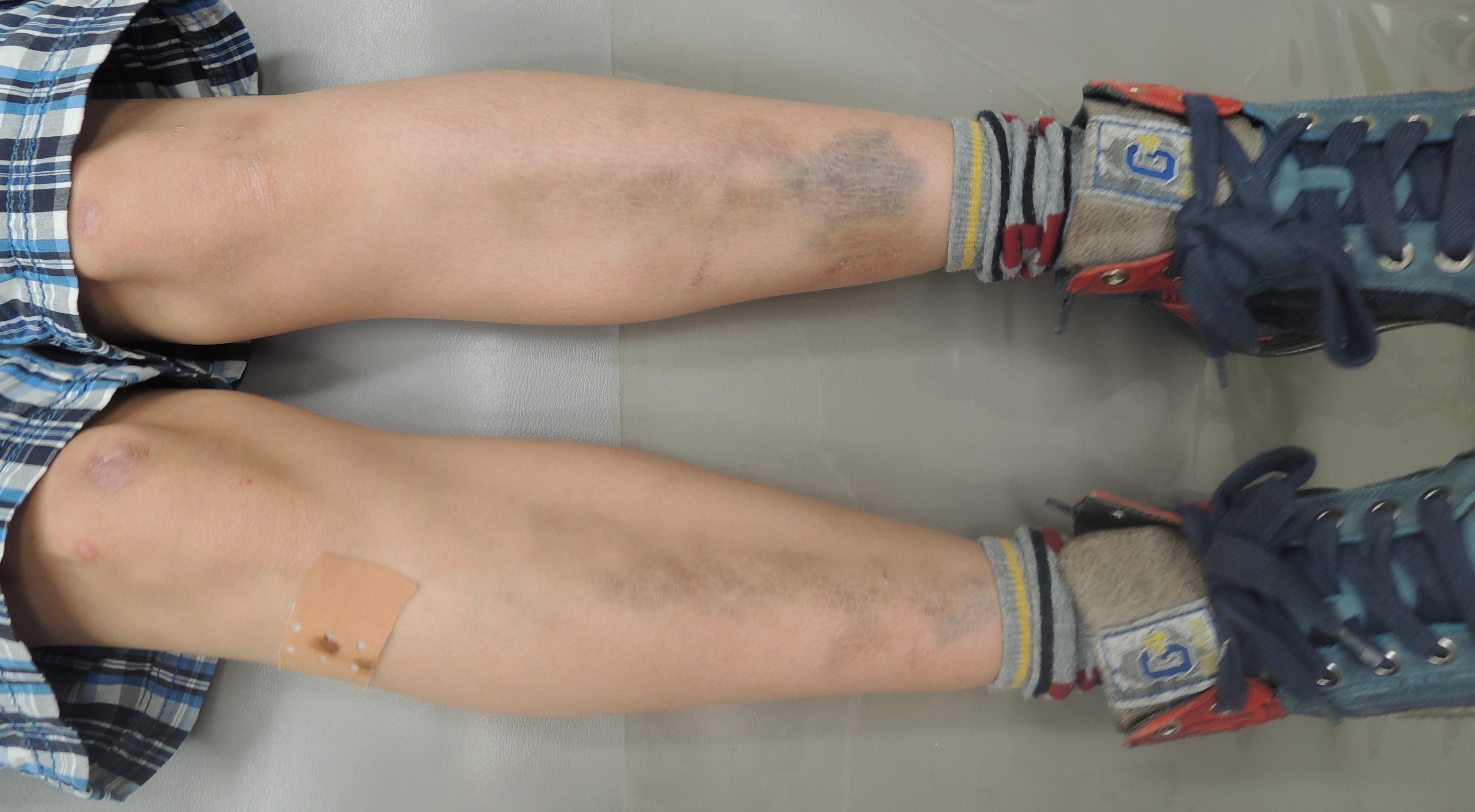
Pretibial hyperpigmentation (child) © Ines Kapferer-Seebacher

Pretibial hyperpigmentation (adult) © Ines Kapferer-Seebacher
For more information please see diagnosis and therapy.