diagnosis
See “downloads“ – site for download content
It is important to state that the specific subtype “periodontal EDS“ is not to be mistaken with a patient suffering from EDS and/with Periodontitis. It is a different sickness and has to be seen differently.
- Major criteria:
- early and severe periodontitis
- lack of attached gingiva
- pretibial plaques
- first-degree relative meeting clinical criteria
- Minor criteria:
- easy bruising
- (distal) joint hypermobility
- skin hyperextensibility and fragility, abnormal scarring (wide or atrophic)
- increased rate of infections
- hernias
- marfanoid facial features
- acrogeria
- prominent vasculature
The minimal criteria suggestive that has to be met for the diagnosis of pEDS consists of major criterion “early and severe periodontitis” or major criterion “lack of attached gingiva” plus at least two other major criteria and one minor criterion.
In addition to that molecular testing is obligatory to reach final diagnosis (4).
Clinical features
Clinical oral features (see periodontal EDS for pictures) of the autosomal-dominant disease periodontal EDS include extensive inflammation of the gingiva as a result of mild dental plaque accumulation as well as early and severe periodontitis that goes hand in hand with rapid destruction of the attachment apparatus at juvenile age (12). This early and severe periodontits is the hallmark of pEDS and with gingival recession the defining clinical feature. If the patients don’t receive periodontal treatment these individuals have a great chance of being edentulous at a mean age of 20 years.
Clinical ORAL features
Early severe periodontitis
The criterion “early severe periodontitis ” is based on periodontal breakdown diagnosed radiologically or clinically at an early age. Mean age of the diagnosis periodontitis in pEDS is 12 years (range 2 – 29 years). First tooth loss due to periodontal reasons was reported at a mean age of 15 years (range 2 – 35 years). Complete tooth loss in pEDS was reported at a mean age of 20 years (range 14 – 48 years). Prepubertal periodontitis at age ≤ 10y was reported in 18.9%(12).

Early severe periodontitis © Ines Kapferer-Seebacher
Gingival recessions
Gingival recessions are the exposure of the tooth roots due to loss of gum and/or retraction of the gum from the tooth crown. It is also known as receding gums. This may cause hypersensitivity as well as a greater mobility of the affected teeth. In addition to these symptoms the teeth will appear longer and spaces between the teeth will grow, the so called black triangles.

Gingival recessions © Ines Kapferer-Seebacher
Lack of attached gingiva
The difference to individuals suffering from chronic or aggressive periodontitis to those from pEDS is the thin and fragile oral soft tissue with missing attached gingiva in individuals suffering from pEDS. This clinical feature eases the clinical diagnosis before signs of periodontitis show. Because of the missing of the attached gingiva the thin and mobile alveolar mucosa continuous directly into the free gingival margin (terminal edge surrounding the tooth), this causes the fragile tissue. Normally this free gingival margin is connected to the attached gingiva which itself is connected to the periostum underneath by collagenous fibrils. This connection is responsible for the protection during chewing or tooth brushing (13).

Lack of attached gingiva © Ines Kapferer-Seebacher
There are a number of specific oral aspects of periodontal EDS which might help to differentiate pEDS from chronic / aggressive periodontitis: Additional oral characteristics of pEDS are:
(1) Severe gingival inflammation in response to mild biofilm accumulation
(2) a striking lack of attached gingiva causing oral tissue fragility
(3) periodontal breakdown without pocketing but severe gingival recession
(4) pattern of alveolar bone loss described as localized to any region, proceeding in a domino effect from one tooth to the next
(5) prominent vasculature on the palate
Clinical EXTRAORAL features
The defining extraoral feature of pEDS is pretibial hyperpigmentation (83%) while other characteristica include easy bruising (96%), skin fragility (83%), and mild skin hyperextensibility (73%).
Joint hypermobility is not a consistent finding (44 %), and if present is mild and often limited to small joints. Joint pain, scoliosis, and pes planus are rare. Abnormal scars (atrophic or wide) are present in 50 % of individuals. Some individuals have additional dermatological findings such as marked facial flushing, thin nails, or thin hair, difficulties in wound healing, with open wounds taking several months to heal.
Forty percent of individuals are prone to recurrent infections such as otitis media, herpes zoster, bladder infections, empyema, kidney infections, or pneumonia. Aneurysms, autoimmune disorders, chronic hoarseness as a result from an abnormality of the cricoarytenoid joint, and organ ruptures have been reported (13).
These pretibial hyperpigmentations are a consequence of easy bruising, delayed wound healing as well as tissue fragility to an injury prone body area. This fragility is often complicated by a variable bleeding tendency. These manifestations have often been misdiagnosed as child abuse, which underlines the importance of gathering detailed family and personal history (14). Leg ulcer is a typical manifestation and may occur within these brownish pretibial plaques because of tissue fragility and delayed wound healing (15).
Beighton-Score (5):
The Beighton-Score can be used for diagnosing joint hypermobility!
A score of 5/9 or greater defines joint hypermobility
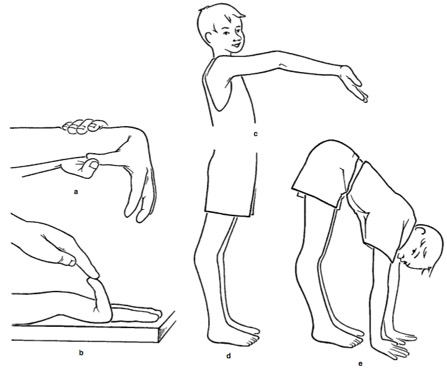
Beighton score © Beat Steinmann
(a) Passive apposition of thumb to the flexor aspect of the forearm; one point for each hand.
(b) Passive dorsiflexion of the little finger beyond 90°; one point for each hand.
(c) Hyperextension of the elbow beyond 10°; one point for each elbow.
(d) Hyperextension of the knees beyond 10°; one point for each knee.
(e) Forward flexion of the trunk with the knees fully extend too that the palms of the hand rest flat on the floor; one point.